
|
Dr. Siegel is currently clinical professor of psychiatry at the UCLA School of Medicine where he is on the faculty of the Center for Culture, Brain, and Development and the founding co-director of the Mindful Awareness Research Center. Dr. Allan Schore is on the clinical faculty of the Department of Psychiatry and Biobehavioral Sciences, UCLA David Geffen School of Medicine, and at the UCLA Center for Culture, Brain, and Development. He is author of four seminal volumes,Affect Regulation and the Origin of the Self, Affect Dysregulation and Disorders of the Self, Affect Regulation and the Repair of the Self, and The Science of the Art of Psychotherapy, as well as numerous articles and chapters. His Regulation Theory, grounded in developmental neuroscience and developmental psychoanalysis, focuses on the origin, psychopathogenesis, and psychotherapeutic treatment of the early forming subjective implicit self. A great introduction to attachment theory given by Dr Richard Bowlby (Dr John Bowlby's son). This short clip contains excerpts from a documentary film on the healing potential of Authentic Movement in working with women recovering from breast cancer. Featuring reflections by Tina Stromsted, Ph.D., it includes footage of research participants exploring natural movement and speaking about their experience. We are naturally born as vital, fully sensory beings. Traumas, tensions, even some education can diminish our vitality, creating unrest and insecurity in our lives. Sensory Awareness -- the practice of deeply exploring our sensations, our actions and interactions, through practical sensing experiments -- can guide us back to our natural resources and lead us to more authenticity and vitality. Through Sensory Awareness we can recover ways of living more fully in the world, rediscovering the wisdom and interconnection of our whole selves and reclaiming our natural being. Trauma is a fact of life. Veterans and their families deal with the painful aftermath of combat; one in five Americans has been molested; one in four grew up with alcoholics; one in three couples have engaged in physical violence—the body keeps the score. That’s how Dr. Bessel van der Kolk, one of the world’s leading experts on developmental trauma, explains how our long-term health and happiness can be compromised by prior exposure to violence, emotional abuse, and other forms of traumatic stress. In his new book, Dr. van der Kolk explores how innovative treatments—ranging from meditation and neurofeedback to yoga, sports, and drama—offer new paths to healing and wellness. A psychiatrist and author of multiple books, his work and perspectives have been featured in The New York Times, on National Public Radio, and in many other media outlets. The fastest way to still the mind is to move the body. Synthesis of the 5Rhythms movement practice developed by Gabrielle Roth in combination with Gestalt therapy and principles from Integrative Body Psychotherapy (IBP). http://www.5rhythms.com/. 5Rhythms transcends dance—movement is the medicine, the meditation and the metaphor. Together we peel back layers, lay our masks down, and dance till we disappear. Dr Edward Tronick speaks about mother-infant attunement and more importantly on disruption of such attunement. From: Polyvagal theory Before I introduce the polyvagal theory, I will first briefly discuss the human nervous system in order to introduce the prerequisites to understanding the polyvagal theory. The human nervous system is divided into two branches; the peripheral nervous system, and the central nervous system (spinal cord). The peripheral nervous system is further divided into somatic-sensory nervous system, and the autonomic nervous system. Somatic nervous system is further divided into motor (efferents), and sensory (afferent) nerves. The autonomic nervous system is divided into two branches, the parasympathetic nervous system and the sympathetic nervous system. The parasympathetic nervous system has two main components: the first branch is controlled by the dorsal vagus nerve, “… characterized by a primitive unmyelinated visceral vagus that controls digestion, and responds to threats by depressing metabolic activities and is behaviorally associated with immobilization and freeze behavior” (Porges, 2001, p. 123). The second branch is controlled by the ventral vagal nerve and is unique to mammals, and according to Porges (2011): The VVC has primary control of supradiaphragmatic visceral organs including the larynx, pharynx, bronchi, esophagus, and heart. […] In mammals, visceromotor fibers of the heart express high levels of tonic control and are capable of rapid shifts in cardioinhibutory tone to provide dynamic changes in metabolic output to match environmental challenges. (p. 160) The other branch of the autonomic nervous system is the sympathetic nervous system (SNS). The sympathetic nervous system is capable of increasing metabolic output and inhibiting the dorsal vagus nerve, thus increasing mobilization behaviors necessary for fight and flight (Porges, 2001). The more primitive life forms use the unmyelinated dorsal vagal complex (DVC), and the sympathetic nervous system to modulate cardiac output and mobilization, or freeze responses. Mammals on the other hand, in order to survive, had to tell the difference and distinguish a friend from a foe, determine and evaluate the safety of their environment, and communicate with their community. Ventral vagus complex (VVC) is the response to these evolutionary needs. The myelinated ventral vagus complex characterizes our social engagement system, which is responsible for facial muscles (emotional), eyelid opening (looking), middle ear muscles (extracting human voice from background noise), muscles of ingestion, muscles of vocalization and language, and head turning muscles (Porges, 2001). In more primitive life forms (pre-mammals), the dorsal vagal complex and the sympathetic nervous system have the opposing functions of decreasing and increasing cardiac output respectively, and thus modulate mobilization. In mammals, with the evolution of the ventral vagal complex, the cardiac output is modulated without the engagement of the former more primitive systems. Thus activation of the myelinated vagal system can result in temporary mobilization and expression of the sympathetic tone without requiring the activation of sympathetic or adrenal system (Porges, 2011). The ventral vagal complex, therefore, acts as a break on cardiac output, capable of rapid changes in heart rate, resulting in mobilizing or calming the individual. Polyvagal theory (Porges, 2011) proposes a hierarchical organization of autonomic nervous system. When a system higher in hierarchy fails, then a more primitive branch of the autonomic system engages. We thus have the following: At the top of the hierarchy is the ventral vagal complex (VVC), a mammalian signaling system for motion, emotion, and communication. The second complex in the hierarchy is the sympathetic nervous system (SNS), which is an adaptive mobilization system engaged during fight or flight behaviors. Finally, the dorsal vagal complex (DVC) is the immobilization system (Porges, 2011). Figure 2 shows the three zones of arousal and the window of tolerance within which the social engagement system (ventral vagal complex) is activated. When someone is hyper-aroused, the person experiences too much arousal to process information effectively, and is usually overwhelmed and disturbed by intrusive images, feelings, affects, and body sensations. When the person is hypo-aroused, he/she experiences something different, namely, a downward modulation of emotions and sensations – a numbing, a sense of deadness or emptiness, passivity, and possibly paralysis. On the other hand, people with a narrow window of tolerance (the middle region in Figure 2), experience fluctuations in emotions and feelings as unmanageable and dysregulating. Most traumatized people have a narrow window of tolerance, and can easily shift into hypo/hyper- arousal states by normal fluctuations in arousal (Ogden, Minton, & Pain, 2006). It is also very important to mention that the states depicted in Figure 2 are not mutually exclusive, in that one can simultaneously be both hyper-aroused, and hypo-aroused – which would be experienced as being highly aroused (ready for action) but unable to move. It is also possible to be in the optimal zone of arousal (activation of our social engagement system) yet experience elements of hypo/hyper-arousal. Also I must note that the boundaries between these zones are not very rigid, and depend on, among other things, emotional state (energetic state) of the mind- body. References Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body. New York, NY: W. W. Norton & Company. Porges, S. (2001). The polyvagal theory: phylogenetic substrates of a social nervous system. International Journal of Psychophysiology, 42, 123-146. Porges, S. (2011). The polyvagal theory. New York, NY: W. W. Norton & Company. Figure 2 Optimal Window of Arousal 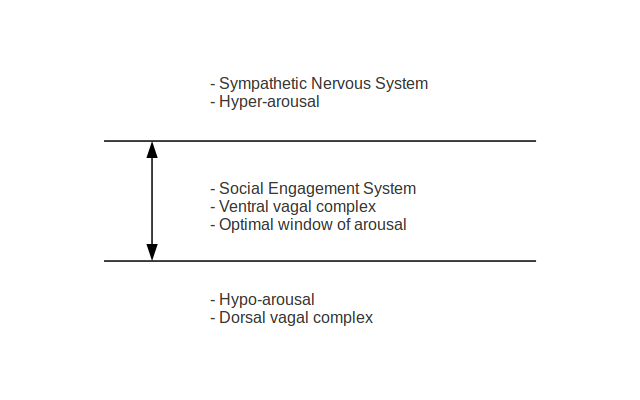 |
AuthorHomayoun Shahri Archives
May 2016
Categories
All
|
 RSS Feed
RSS Feed